Case:
A 23-year-old male with recent past medical history of GSW to R chest two weeks ago. At that time he had an equivocal pericardial window on his FAST and, given the trajectory near the heart, went to the OR for a pericardial window which was negative. He developed postoperative pericarditis and an echo showed a trivial effusion with no other findings. He was treated with NSAIDs/colchicine and discharged.
He returned to the ED one week later with worsening dyspnea and pleuritic chest pain. Initial vitals were notable for tachycardia with a normal BP. The patient was uncomfortable appearing. His midline chest incision appeared clean, dry, and intact. A POCUS was performed and demonstrated the following:
Case Conclusion:
The POCUS performed in the ED showing a loculated pericardial effusion and early-diastole RV wall intrusion was concerning for tamponade physiology. Given his tachycardia and the findings on the echo, the patient went for a percutaneous pericardiocentesis with 500 mL of serosanguinous fluid removed. The patient did well postoperatively and was discharged on continued colchicine/ibuprofen.
Tamponade on Ultrasound:
While tamponade is ultimately a clinical diagnosis, echo is a central component of the workup. Focus on the right heart - since pressures are lower, these chambers will be the first overwhelmed by the increasing pressure exerted from the accumulation of pericardial fluid. Tamponade occurs when the pressure in the pericardial sac overwhelms RV pressure, impeding sufficient cardiac filling during diastole and ultimately affecting hemodynamics.
The earliest and most sensitive tamponade physiology is late-diastole R atrium collapse. This can occasionally be seen in other pathologic states such as hypovolemia. The next finding that develops is the collapse of the free wall of the RV during early diastole. Remember back from medical school (!!) that most of the filling of the ventricle occurs during early diastole as the heart is very compliant to increases in pressures at this point in the cardiac cycle. Thus, impeded filling of the RV during early diastole will ultimately limit cardiac output. This finding is less sensitive but more specific for tamponade.
Other echo findings consistent with tamponade are a dilated IVC whose diameter does not significantly vary with respiration. This finding is sensitive for tamponade but will occur with any condition causing elevated R pressures. Abnormal septal motion (right bowing into left during diastole) may also be seen.
While not a necessary component of the EMBU to diagnose tamponade physiology, you can also use pulsed-wave Doppler to visualize pulsus paradoxus. In the apical 4-chamber view, obtain tracings of either the mitral valve or tricuspid valve. There is normally not much variation in the velocity of blood flow across the valve in diastole. In tamponade, regular flow variations with respirations are exaggerated since the cardiac chambers are smaller and unable to fully expand. Variation of maximum velocity flow across the valve >25% during inspiration is consistent with tamponade:
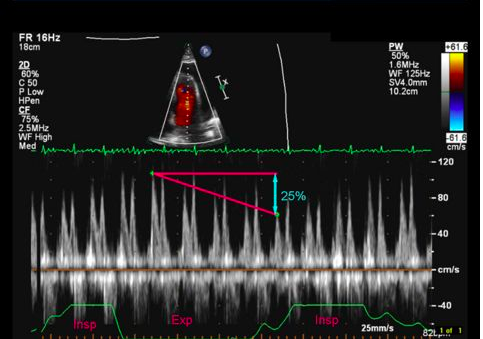
(image from http://web.stanford.edu/group/ccm_echocardio/cgi-bin/mediawiki/index.php/Tamponade)
- Jessica Patterson, MD, Emergency Medicine Ultrasound Fellow
References
1. https://www.acep.org/_Ultrasound-Section-Microsite/Cases-That-Count-(Cardiac-Tamponade)/#sm.0001w7yw6cwacdipw3t1od3b3mvza
2. https://www.ncbi.nlm.nih.gov/pubmed/12784745
3. http://journal.chestnet.org/article/S0012-3692(17)33071-4/pdf
4. http://web.stanford.edu/group/ccm_echocardio/cgi-bin/mediawiki/index.php/Tamponade